
I'm going to prefix this post with a complaint. One of the biggest annoyances in my professional life is the misnomer that is the term 'O2 stats'.
It's sats. As in saturation. Not status.
Measurement of Oxygen Saturation or SpO2 is an extremely common assessment that is now performed routinely by nurses, doctors and paramedics. SpO2 is indicative of effectiveness of respiration by quantifying perfusion. Essentially this devices spits out a percentage that tells us how on average at what oxygen carrying capacity our red blood cells are.
That's great, but what does this 'oxygen saturation' mean to us? and how can this number really be used effectively?
We're going to explore the sat, it's meaning, it's use and really get intimate with the nuances that is oximetry.
SpO2 vs SaO2... Whats the difference?
These two terms are often (unfortunately) used interchangeably, however the both refer to two different modalities of measurement. This bit is really important in understanding the implications of SpO2 and it's relation to hypoxia.
- SpO2 refers to peripheral measurment of oxygen saturation, this measurement is non-invasive.
- SaO2 refers to an arterial measurment of oxygen saturation, this measurement is invasive and requires an ABG or artline.
That's how I remember it.[1]
Why do we measure oxygen saturation?
Plainly, because we can. SpO2 in routine assessment of vital signs is not necessary, it is however extremely helpful in identification of deterioration (or improvement). Oximetry makes things easier for us. It gives us a number to slap on dysponea. How often have you heard;
'This bloke has come in with shortness of breath, his sats were sitting about 92% on room air, so we've put him on a couple of litres, bringing his sats up to 97%.'Personally, I have a couple of issues with sweeping statements like this, but we'll bypass those and look at this situation. Our patient has come in experiencing what he describes as shortness of breath. We've taken this subjective observation, or symptom and made it objective.[2]

Physiologically, we know that oxygen is transported throughout the body by red blood cells - specifically, heamoglobin. Haemoglobin have binding sites for oxygen molecules to attach. Haemoglobin are considered Oxygen Saturated when they are carrying their full capacity of oxygen.
Measurement of Oxygen Saturation A.K.A Pulse Oximetry, A.K.A SpO2 averages the number of oxygen binding sites of haemoglobin that are occupied and gives us a percentage.
So consider it this way;
10 Taxis arrive at a night club simultaneously, to pick up the waiting drunken revelers. There are 40 inebriates. Amazing. That's a perfect number. So, all 40 of our partiers get in a cab and travel to next club - 100% occupancy of the cabs!
After a few hours and drinks at the next club our 40 hooligans are ready to go again, however, of our 10 cabs, some of drivers refuse to take particularly pickled people. So, The actual capacity of the 10 taxis is 40 people, however, only 36 of the seats are being used effectively, therefore we have a 90% occupancy.
Now swap the word Taxi for Haemoglobin, and the various references to club-goers for Oxygen and you get a really bare bones example of what oximetry measures.
Oxy-Haemoglobin Disassociation Curve
There exists a visual representation of how effective haemoglobin is at carrying oxygen molecules, referred to as the Oxy-Haemoglobin Dissasociation Curve. To understand this curve, we need to understand a little about the relationship between Oxygen Saturation, and the Partial Pressure of Oxygen (PO2).
So in the above example, We'll add another factor - Intoxication level. As the intoxication increased, the ability to use the cabs decreased - This is PO2.
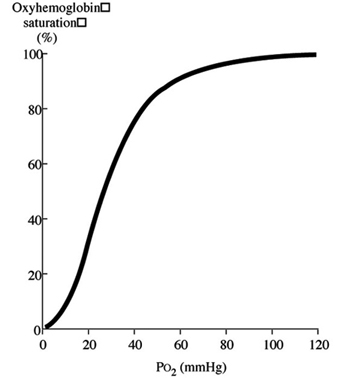
PO2 directly correlates with the affinity of oxygen to haemoglobin, The higher the PO2, the Higher the Saturation.
Whilst it's a little difficult to see in the above image, an SpO2 of 92% will result in a PO2 of 60mmHg and an SpO2 of 89% will result in a PO2 of 50mmHg*, and if you follow the graph, that oxygen affinity only decreases more exponentially - thus decreasing circulating oxygen.
*These numbers, of course assume optimal health and condition of the person.
Left and right shift of the curve i.e. standard deviations, occur for various reasons from alterations in temperature, PCO2 levels, and Blood Hydrogen levels, and can affect the affinity and dictate interventions required. [3]
Key Points to this stage:
- SpO2 is non-invasive measurement of oxygen saturated Hb.
- SpO2 gives is a tool to objectively measure respiratory complaints.
- SpO2 correlates to PO2, Which dictates the affinity of oxygen to Hb.
- The Oxy-Hb Curve can shift, based on physiological alterations.
Putting it to work
So, let's put this to work. We now know that the partial pressure of oxygen PO2 is what dictates oxygen molecules affinity to Haemoglobin, and we know that PO2 directly correlates with SpO2. So we can use this knowledge to direct our clinical assessment and judgement on oxygen requirements of this patient.
Most sources agree that SpO2 should be targeted at 94%-99% in a healthy adult. So we can use this as basis for oxygen titration, using different delivery devices we can alter how much oxygen we deliver (FiO2).[1,4]
Can too much oxygen really be bad?
Yes. SpO2 does not exceed 100%. PO2 however, does. In some circumstances, such as CO2 retention, seen in COPD. there is a left shift in the Oxy-Hb curve. This results in an increased O2 affinity for Hb, (PO2) At lower levels of SpO2.
It was previously thought that increasing SpO2 increases PO2 which can slow hypoxic drive, decreasing respiratory effectiveness, and have the opposite of intended effect, however, recent studies have found that CO2 retainers do not rely on hypoxic drive to breath.
The result of CO2 retention has been attributed to chronic, increased V/Q mismatch (Ventilation/Perfusion). The administration of supplementary oxygen, particularly high flow oxygen causes a reversal of the increased V/Q mismatch, resulting in hypoxaemia.
Essentially, there are two types of alveoli - those with good ventilation (V) and those with poor ventilation. An alveolus with good ventilation will generally have a poorer perfusion (Q) where as a poorly ventilated alveolus will have good perfusion. This is V/Q mismatch. - The more oxygen, the less circulation - this is achieved by vasoconstriction.
In COPD alveoli have impaired gas exchange ability, as a protective measure the localized vasoconstriction to the capillary supplying the alveolus occurs. When oxygen is administered, this protective measure is reversed as the alveoli ventilation is increased, However, due to impaired gas exchange, the ability for the oxygen to effectively diffuse to haemoglobin is decreased, resulting in increased oxygen, and decreased CO2 in the alveolus. This is known as 'Dead space ventilation'.[5]
BUT, This CO2 retention requires an assessment of Arterial Blood Gases to diagnose, and only upon confirmation of CO2 retention should modifications to the SpO2 target range be made.
In unconfirmed cases, where the patient is acutely short of breath, with SpO2 <94% Oxygen should still be given as per facility/service protocol. [1,4]


In modern health care, oximetry forms part of a respiratory assessment. It supplements respiratory rate, assessment of respiratory effort, chest auscultation and other technologically challenged assessment measures. SpO2 is a fantastic tool when used with a good understanding, and used correctly. It's an essential piece of kit in Critical Care and is fast becoming an essential routine assessment. [2]
Can too much oxygen really be bad?
Yes. SpO2 does not exceed 100%. PO2 however, does. In some circumstances, such as CO2 retention, seen in COPD. there is a left shift in the Oxy-Hb curve. This results in an increased O2 affinity for Hb, (PO2) At lower levels of SpO2.
It was previously thought that increasing SpO2 increases PO2 which can slow hypoxic drive, decreasing respiratory effectiveness, and have the opposite of intended effect, however, recent studies have found that CO2 retainers do not rely on hypoxic drive to breath.
The result of CO2 retention has been attributed to chronic, increased V/Q mismatch (Ventilation/Perfusion). The administration of supplementary oxygen, particularly high flow oxygen causes a reversal of the increased V/Q mismatch, resulting in hypoxaemia.
Essentially, there are two types of alveoli - those with good ventilation (V) and those with poor ventilation. An alveolus with good ventilation will generally have a poorer perfusion (Q) where as a poorly ventilated alveolus will have good perfusion. This is V/Q mismatch. - The more oxygen, the less circulation - this is achieved by vasoconstriction.
In COPD alveoli have impaired gas exchange ability, as a protective measure the localized vasoconstriction to the capillary supplying the alveolus occurs. When oxygen is administered, this protective measure is reversed as the alveoli ventilation is increased, However, due to impaired gas exchange, the ability for the oxygen to effectively diffuse to haemoglobin is decreased, resulting in increased oxygen, and decreased CO2 in the alveolus. This is known as 'Dead space ventilation'.[5]
BUT, This CO2 retention requires an assessment of Arterial Blood Gases to diagnose, and only upon confirmation of CO2 retention should modifications to the SpO2 target range be made.
In unconfirmed cases, where the patient is acutely short of breath, with SpO2 <94% Oxygen should still be given as per facility/service protocol. [1,4]
Limitations of Pulse Oximetry
This is the part where this fantastic tool loses it's appeal.
- Poor Peripheral circulation, e.g. Peripheral Vascular Disease
- Cold peripheries
- Nail Polish
- Excessive Movement
- Arrhythmia
- Anaemia, including Sickle Cell Disease
- Jaundice
- Hypovolaemia
- Light levels in environment
can all cause inaccurate measurements. [6]
So, how do we determine if our SpO2 reading is accurate? Accompanying the SpO2 reading on the pulse oximeter should be a plethysmograph, or pleth waveform.
This waveform should be regular and rhythmic. Low frequency waves may indicate a poor reading due to any of the above reasons.
A one off O2 Sat, like any other vital sign provides very little information, SpO2 trends provide good indication as to the effectiveness of respiration and/or interventions.
In modern health care, oximetry forms part of a respiratory assessment. It supplements respiratory rate, assessment of respiratory effort, chest auscultation and other technologically challenged assessment measures. SpO2 is a fantastic tool when used with a good understanding, and used correctly. It's an essential piece of kit in Critical Care and is fast becoming an essential routine assessment. [2]
Important side note - all above values represent measurment at relative sea level.
If you want to look into the effects of altitude on respiration do some research into Boyle's Law and Gongs Nomogram.[7]
Key Points to take home:
Oxygen should be delivered based on SpO2 trends and should be titrated to those trends
SpO2 measurement has limitations. These limitations must be considered when putting interventions in place, based on SpO2.
Low SpO2 (<94%) should always be treated, despite diagnosis - the exception to this is CO2 retention seen in COPD and confirmed by ABG. In this case saturation targets should be modifed.
References
[1]Queensland Health, Royal Flying Doctor's Service. (2013). In Primary Clinical Care Manual.
[2]Elliott, M., & Coventry, A. (2012). Critical care: the eight vital signs of patient monitoring. British Journal Of Nursing, 21(10), 621-625.
[3]Morgan TJ. (1999) The oxyhaemoglobin dissociation curve in critical illness. Crit Care Resusc. 1(1):93-100.
[4]Ambulance Victoria (2014) Ambulance Victoria, Clinical Practice Guidlines
[5]Abdo WF, Heunks LM. (2012) Oxygen-induced hypercapnia in COPD: myths and facts. Crit Care. 2012 16(5):323.
[6]Nickson, C (2013) Life in the Fast Lane – pulse oximeter (Blog post).http://lifeinthefastlane.com/education/ccc/pulse-oximeter/
[7]Greater Sydney Area HEMS (n.d.)Air Medical Issues (Blog Post). http://sydneyhems.com/resources/curriculum/air-medical-issues/
No comments:
Post a Comment